It’s being called the worst pandemic in modern history. I’m not talking about COVID-19 — thought it most certainly applies here too — I’m talking about the dangerous, disturbing and even deadly spread of misinformation online.
You can’t go on Facebook, YouTube, Twitter — to name a few — without seeing examples of it all over the place, from people reposting old photos as if it’s current news and information to the more nefarious trolls, bots, deepfakes, and online agitators.
No matter how much big tech companies and others pledge to contain this toxic spread, it’s up to us to actually do something about it.
TAKE A LOOK AT YOUR OWN FEEDS
We’ve all done it — spotted that headline, photo, or emotional post from someone’s uncle or “friend,” that underscores everything we already think and feel — and passed it on. It’s human nature. Add a pandemic, failing trust in authority figures, feelings of fear and lack of control — all while stuck at home, and we have a perfect storm for an infodemic.
“The environment created by the pandemic has bred a multitude of falsehoods even as truth has become a matter of life and death,” writes the authors of a new paper in Psychological Science who investigated why people believe and spread false information about COVID-19. “In the case of COVID-19, this misinformation comes in many forms — from conspiracy theories about the virus being created as a biological weapon in China to claims that coconut oil kills the virus.”
The fix, however tempting, is not to fight with, or shame people in social media circles, nor is it as easy as pointing people toward the truth. “Turning around those who buy into false information is not as simple as piercing epistemic bubbles [sic] with facts,” Christopher Robichaud, senior lecturer in ethics and public policy at Harvard Kennedy School told the Harvard Gazette recently.
I took a peek at one of my childhood friends’ Facebook feeds and spotted 16-times he’s shared a debunked conspiracy theory, cheapfake video, or politically-charged falsehood. He’s one of only a handful of people I haven’t already “Unfriended” over misinformation — because I know he doesn’t do it knowingly or maliciously — and I’m cautiously optimistic that non-judgemental nudges (like this column) will help him and others flatten this curve of confusion.
With that goal in mind, here’s what we know so far is true, and what we know is not, followed by recommendations on how to tell the difference.
FIVE TRUTHS ABOUT COVID-19
- TRUE: What we know about COVID-19 is changing rapidly
If it feels like there’s a new coronavirus symptom, warning, or mandate popping up on your newsfeed almost every day, it’s because there is. COVID-19 is a new disease, and countless scientists, researchers, and health experts are studying it every day. That means a flood of information that is often difficult to parse.
“Information overload is incredibly anxiety-provoking—which is true even when the information is accurate,” Jaimie Meyer, MD, MS, says. Meyers is a Yale Medicine infectious diseases specialist concerned that poor information only makes things worse. “If people get the wrong information from unreliable sources, we may have more trouble slowing the spread of the virus. And we can’t afford to get this wrong.”
Meyers and other health experts suggest turning to official information channels like the World Health Organization’s daily “Situation Reports,” which offer up-to-date info on the progress of the pandemic and news that you can actually trust.
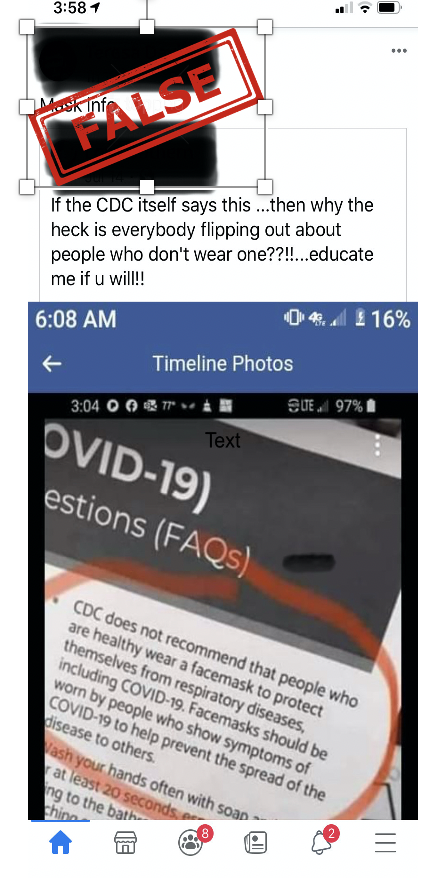
- TRUE: Masks help slow the spread of COVID-19
Robert Redfield, the Centers for Disease Control and Prevention, said last month, that the U.S. could get the virus “under control” within four to eight weeks if everyone wore masks. The CDC also said that even cloth face coverings help prevent people who have COVID-19 from spreading the virus to others.
“We are not defenseless against COVID-19,” Redfield added. “Cloth face coverings are one of the most powerful weapons we have to slow and stop the spread of the virus – particularly when used universally within a community setting. All Americans have a responsibility to protect themselves, their families, and their communities.” In addition to masks — social distancing, washing your hands, and disinfecting surfaces — remains the most effective ways of slowing the virus.
- TRUE: COVID-19 has a wide range of symptoms
No matter how outlandish it might seem, it’s true that COVID-19 tackles the body in weird and widespread ways. While initially thought to be a strictly respiratory illness, we now know that it appears to have the ability to invade nearly every major organ. Symptoms can range from the slightly more expected fever, cough, nausea, headaches, and shortness of breath — to a loss of taste and smell, blot clots, rashes, swelling, kidney or liver damage, or strokes. Even more confusing? Some people infected with the virus show no symptoms at all.
- TRUE: Children can get critically ill from COVID-19
When it comes to children and COVID-19, news headlines in February and March often wondered if the virus even impacted youngsters at all. The answer is: yes, it can — and does. It’s true that so far, children often don’t get as sick as adults, but according to the CDC, people of any age with certain underlying conditions, such as type diabetes, are at higher risk of serious illness with COVID-19. Additionally, children with neurologic, genetic, metabolic conditions, or who have congenital heart disease might be at increased risk for severe illness from COVID-19 compared to other children. And yes, children are dying from COVID-19 too.
One recent study published in the JAMA Pediatrics also suggests infected children can carry a high viral load of the coronavirus in their noses and throats — as much as infected adults. They also found that kids younger than the age of five may host up to 100 times as much of the virus in the upper respiratory tract as adults. These new findings might shed light on how children can pass the virus on to adults, and potentially develop other conditions tied to the virus later.
- TRUE: We don’t know the exact number of COVID-19 cases and death rates in the U.S.
If I had a dime for every person who shared false information around hospitals, local and national authorities are “inflating COVID-19 death tolls for money or political reasons” — I would be a wealthy gal. It’s true that keeping track of COVID cases and death rates isn’t like keeping the score of a baseball game. But so far, several studies and analysis lead toward under-reporting, not the other way around.
On it’s website, the CDC explains it uses diverse data streams to track and analyze COVID-19 at the local, state, and national levels. These figures are updated daily on its cases in the U.S. web page. There is so much misinformation spreading around facts, figures, and case numbers that the CDC also has a detailed FAQ on this information is gathered, calculated, and reported.
FIVE LIES ABOUT COVID-19
- FALSE: Masks don’t help/Wearing a mask is dangerous
One of the biggest myths — turned political lighting rods of this entire pandemic — is that masks don’t do anything to halt the spread of the coronavirus. This particular falsehood has its roots in some early advice from health officials who claimed that only those who were already infected with the virus should wear masks. This advice was well-meaning — meant to lessen the strain on supplies of masks so that healthcare workers could actually get the equipment they needed — but it mutated into a misinformation campaign that continues today. The truth, tweeted by the President of the United States himself last week, is that everyone should be wearing a mask in places where they will be in even remote contact with other people, including stores and even parks.
Also false in the commonly shared misinformation around masks is that they’re dangerous. Wearing medical masks for long periods may be uncomfortable for some, but it does not cause oxygen deficiency or cause too much carbon dioxide to build up in the bloodstream (CO2 intoxication), according to WHO. The same applies for N95 masks and cloth face coverings, according to Healthline. These widely-spread myths have been debunked many times in the past few months, yet they still persist across social media.
Masks do not increase your risk of coming down with COVID-19 either. These rumors seem to have their roots in the misguided belief that using a facemask in public places will cause your mask to be saturated with the virus, potentially increasing your risk of infection when you take it off or touch it. Others seem to think that using a face mask causes your oxygen level to decrease, posing other dangers.
The truth, of course, is that masks are still the best way to combat a coronavirus infection. “We don’t have ERs full of people who wore a mask and became sick because they were wearing a mask,” William Schaffner, an infectious diseases specialist at Vanderbilt University Medical Center, said in a statement. “The big issue with masks is that people aren’t wearing them.”
- FALSE: COVID-19 is no worse than the flu
It’s okay to offer reassurance to people who may be panicking, but to claim that COVID-19 is basically just “the flu” is both dangerous and completely untrue. Facebook has been a hotspot of people spreading this myth, and you don’t have to search far to find a lot of misleading information. There are countless posts that include cherry-picked data, citing information that doesn’t show the whole picture of the outbreak. Though the death rate for COVID-19 is unclear (and potentially as much as higher than reported according to several recent studies), almost all credible research suggests it is much higher than that of the seasonal flu, which has a death rate of around 0.1% in the U.S.
There are many key differences between the flu and COVID-19, including the fact that people can remain symptom-free for up to two weeks after being infected, and are contagious during that entire time period. On top of that the novel coronavirus appears to have a significantly higher mortality rate, according to the World Health Organization. So, it spreads easier and kills more people when compared to the flu, which are obviously very important distinctions.
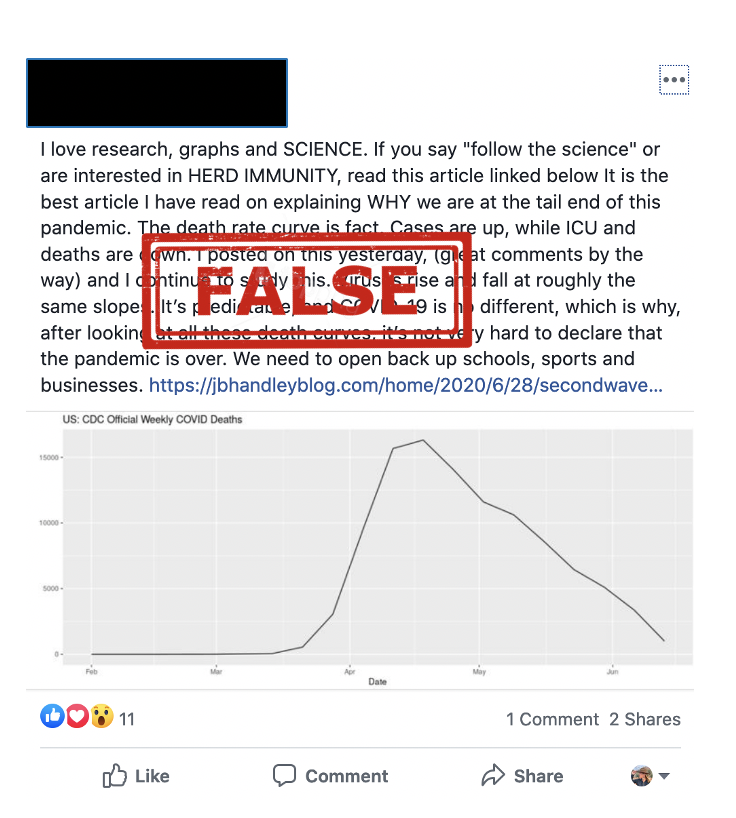
- FALSE: We are at the tailend of this pandemic
More than 17.3 million coronavirus cases have been recorded worldwide, including at least 673,800 deaths, according to Johns Hopkins University. Cases of COVID-19 in the United States continue to increase as well — the U.S. case count is now more than 4.6 million and the death toll more than 1504,000. What’s more, a key coronavirus model now projects there will be more than 230,000 deaths in the U.S. from Covid-19 by November — up 11,000 from its previous forecast. Suffice it to say, the pandemic is far from over.
- FALSE: COVID-19 escaped from a lab
My family just had this discussion around the dinner table the other night. One of uncles made a compelling argument around the notion that COVID-19 is a man-made bioterrorist weapon that “accidentally” escaped from a lab.
Fear and anger are often siblings, and in the case of the coronavirus, the fact that it seemingly “came out of nowhere” led some to blame the pandemic on scientists who must have created the virus and then accidentally (or perhaps purposefully) released it on the public. But the truth is, there’s no evidence to support this theory. According to a report by Live Science, “SARS-CoV-2 closely resembles two other coronaviruses that have triggered outbreaks in recent decades, SARS-CoV and MERS-CoV, and all three viruses seem to have originated in bats. In short, the characteristics of SARS-CoV-2 fall in line with what we know about other naturally occurring coronaviruses that made the jump from animals to people.”
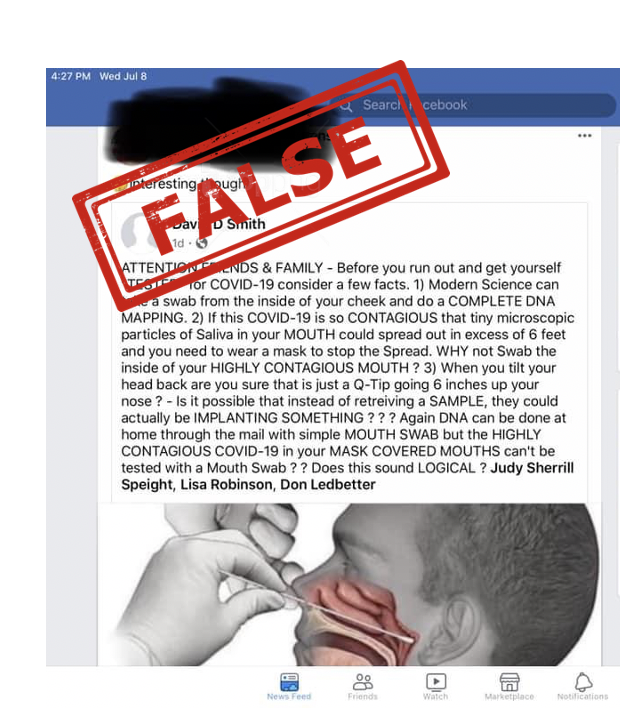
- FALSE: Coronavirus tests cause brain damage or plant substances on the brain
Here’s another one the childhood friend I mentioned above shared, along with hundreds of thousands of other people around the globe. USA Today has already debunked the falsehood that those deep nasal swabs used to test for COVID-19 take samples from the cribriform plate (the roof of the nasal cavity), and can therefore be used to plant chips, viruses or chemicals on the brain, “stealing” DNA, and potentially causing brain damage.
Reality is pretty simple around this one: Nasopharyngeal swabs collect samples from the nasopharynx — just above the soft palate — from where it’s not anatomically possible for them to plant anything onto the brain. Also, USA Today tracked down the man who originally posted this theory, and he admitted “that he came up with the post with ‘a couple drinking buddies,’ and did not provide sources to back up the claims, saying “the post was ASKING QUESTIONS about Implementation not Stating Facts.”